2.1 Include child and adolescent health in initial health assessment
Key agencies should initiate a coordinated needs assessment at the start of a humanitarian emergency to provide an understanding of the crisis, including how it may continue to develop, and identify gaps in response and any operational constraints. This assessment should consider both the crisis impact (scope and scale of the crisis, how people are affected) and the operational environment (capacities, humanitarian access) (Fig. 8).
The IASC operational guidance for coordinated assessments in humanitarian crises (25) describes four phases of the initial assessment (Fig. 9). OCHA typically leads the first two phases, using the multi-sector initial rapid assessment (MIRA) tool (26) (including the rapid health assessment). The later phases require a more tailored plan and are typically coordinated within particular sectors/clusters (Box 7).
The health cluster will lead the rapid health assessment and contribute to other parts of the multi-sector initial rapid assessment (MIRA) tool. The rapid health assessment will address:
- health status and risks,
- health resources and service availability
- health system performance (including coverage, quality, access and utilization).
The RMNCAH/CAH working group, and individual agencies, should actively participate to ensure that children and adolescents are counted and assessed accurately. This starts with disaggregating data by age (newborns, < 5 years, 5–9 years, 10–14 years and 15–19 years). In many cases, there will be specific CAH vulnerabilities and risks (Box 8), capacities and actions that need to be addressed within a needs assessment.
As much as possible, integrate child and adolescent needs assessment activities within the broader needs assessment activities. Commonly used data collection tools are described in Table 2.
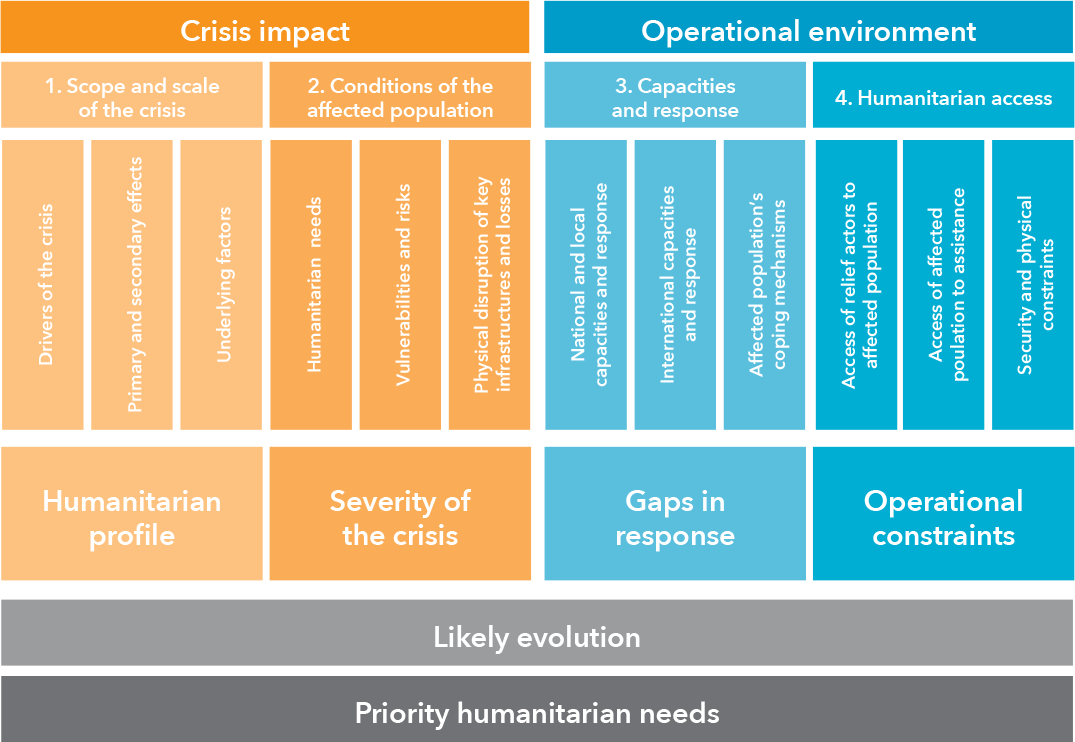
Fig. 8 Components of a needs assessment (26)
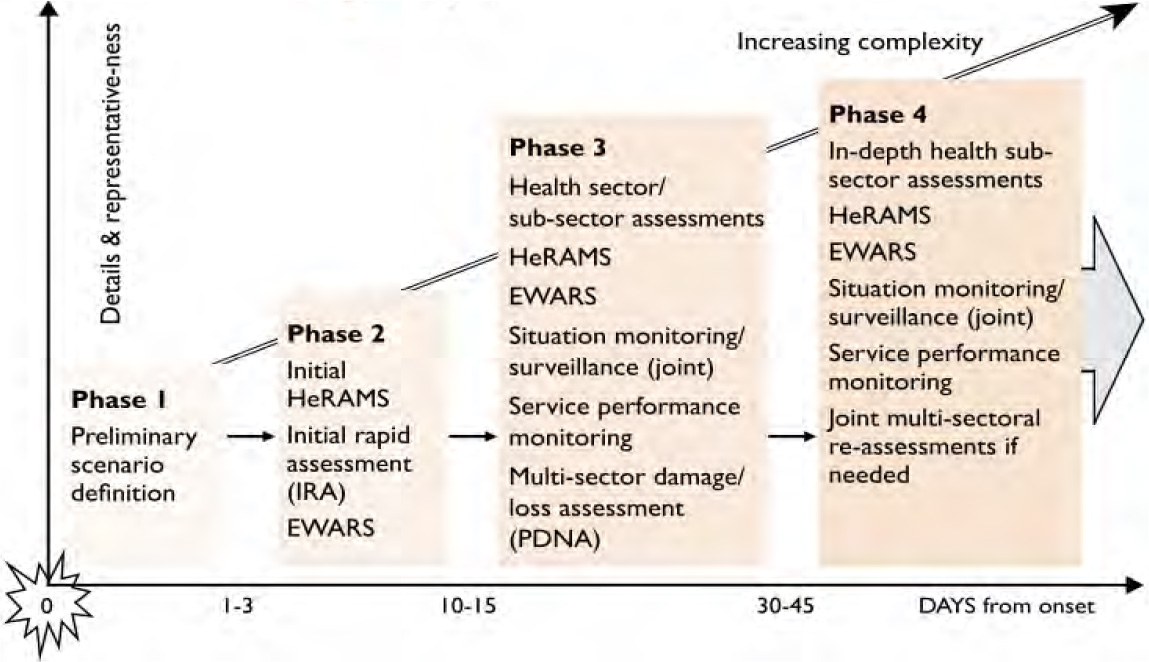
Fig. 9 Coordinated assessment and phases (HeRAM: Health Resources Availability Monitoring System, EWARS: Early Warning, Alert and Response System, PDNA: post disaster needs assessments) (25)
Box 7 Ten principles for conducting needs assessments (25)
- Wherever possible, assessments are led by national governments and promote ownership by national and local authorities.
- Plan for assessments as part of emergency preparedness.
- Build each assessment on existing data, assessing CAH information from existing quantitative and qualitative data, e.g. pre-crisis national demographic surveys and reports from previous emergency responses.
- Ensure links between assessment and monitoring.
- Collect exactly the data required for decision-making.
- Involve all stakeholders in assessment design and implementation. Consider the use of technology, including social media, to reach young people.
- Address priority issues and groups, including gender, age, disability, unaccompanied minors, ethnic minorities and other groups at high risk.
- Use sound information management strategies.
- Include an analysis of context.
- Do assessments with future recovery and development activities in mind.
The health cluster will lead the rapid health assessment and contribute to other parts of the multi-sector initial rapid assessment (MIRA) tool. The rapid health assessment will address:
- health status and risks,
- health resources and service availability
- health system performance (including coverage, quality, access and utilization).
The RMNCAH/CAH working group, and individual agencies, should actively participate to ensure that children and adolescents are counted and assessed accurately. This starts with disaggregating data by age (newborns, < 5 years, 5–9 years, 10–14 years and 15–19 years). In many cases, there will be specific CAH vulnerabilities and risks (Box 8), capacities and actions that need to be addressed within a needs assessment.
As much as possible, integrate child and adolescent needs assessment activities within the broader needs assessment activities. Commonly used data collection tools are described in Table 2.
Box 8 Children at high risk in emergencies and specific issues to consider
Children at high risk
- Young children
- Girls
- Undocumented migrants, unaccompanied and separated children
- Children and adolescents from ethnic or religious minority populations
- Children and adolescents with disability or chronic health conditions
- Child and adolescent caregivers or primary income earners
- Children and adolescents in the armed forces (and ex-combatants) or justice system
- Children and adolescents in forced or exploitative labour, including sex work
- Child and adolescent survivors of physical, sexual and emotional abuse
Issues to consider
- Violence, trauma: particularly common in armed conflict, displaced populations and natural disasters
- Food insecurity, undernutrition: particularly common in famine, armed conflict and displaced populations
- Disease outbreaks: particularly common in displaced populations and refugee camps, and in the case of destruction of water and sanitation infrastructure or low immunization coverage
- Uncontrolled endemic disease: particularly common in displaced populations, and in the case of destruction of social and health infrastructure
- Mental health and psychological well-being: particularly common in armed conflict and protracted emergencies
- Gender: effect of the emergency on girls and boys
Table 2 Data collection tools commonly used in humanitarian emergencies
Data collection method |
Comments |
IASC Multi-sector initial rapid assessment (MIRA) tool (26) |
MIRA is the coordinated approach to overall assessment of a crisis situation, and is led by OCHA. It includes the rapid health assessment which is led by the health cluster. |
WHO Health Resources Availability Monitoring System (HeRAMS) (27) |
HeRAMS is a tool for initial assessment and ongoing monitoring of human resources for health, and is used by the health cluster. |
WHO service availability and readiness assessment (SARA) (28) |
SARA is an alternative tool for cross-sectional assessment of health service availability and readiness. |
WHO rapid risk assessment (29) |
Rapid risk assessment guides the initial rapid assessment of acute public health events. |
WHO Early Warning and Response System (EWARS) (30) |
EWARS is a system for early detection of crises. (See also action area 3 – Monitor, Evaluate, Review) |
3W/4W/5W (31) |
This tool assesses humanitarian response: who, what, when, where, and for whom. |
WHO strategic tool for assessing risk (32) |
The WHO strategic tool for assessing risk is mainly used for planning (preparedness). |
SMART nutrition assessment (33) |
SMART is a method for rapid assessment of nutrition in emergencies. |
Key actions – needs assessment
Adapted from the Sphere Health Standards (1)
- Members of the RMNCAH/CAH working groups review the OCHA risk profile, all hazards response plans and other relevant sources of information.
- Contribute to a systematic, objective and ongoing assessment of the context and stakeholders (intersectoral).
- The RMNCAH/CAH working group coordinates input from agencies to ensure that CAH concerns are fully represented in the rapid health assessment (and all future assessments).
- Advocate for disaggregation of data by sex and age (newborn, < 5 years, 5–9 years, 10–14 years and 15–19 years).
- Use pre-existing data as much as possible (e.g. service coverage, and morbidity and mortality). Coordinate with others to avoid burdening communities with multiple assessments, and unnecessary duplication.
- The RMNCAH/CAH working groups contribute to assessing the safety and security of affected, displaced and host populations to identify threats of violence and any forms of coercion, denial of subsistence or denial of basic human rights – with a focus on children and young people.
- Consider using the Child protection rapid assessment toolkit (34) to assess child and adolescent risks, vulnerabilities and needs.
- Consider how gender roles, norms and stereotypes affect children’s and adolescents’ experience of and response to a crisis. Consider how to approach this in your programmes and activities.
- Share assessment findings widely (including with affected populations). Use multiple communication channels (e.g. face-to-face, email, social media and radio).
Key indicators – needs assessment
- The health sector lead agency has conducted an initial rapid assessment, with active involvement of the RMNCAH/CAH working group.
3 Check with your country coordinators and online (https://reliefweb.int/).